Menu
M. Miyashita, Z.C. Narita, J. Devylder, S. Yamasaki, S. Ando, K. Toriumi, S. Yamaguchi, M. Nakanishi, M. Hosozawa, S. Koike, K. Suzuki, K. Baba, J. Niimura, N. Nakajima, D.M. Anglin, G. Knowles, C. Morgan, M. Richards, M. Hiraiwa-Hasegawa, T.A. Furukawa, K. Kasai, A. Nishida, M. Arai, Examining glycation as a mediator linking bullying to psychotic experience and depressive symptom in adolescents, Mol. Psychiatry. (2026).
https://doi.org/10.1038/s41380-026-03521-7
Adolescent bullying victimization is known to increase the risk of psychiatric symptoms such as psychosis-like experiences [1] and depressive symptoms [2].
However, the biological mechanisms through which bullying, as a form of social stress, leads to psychiatric symptoms had not been fully elucidated.
Advanced glycation end products (AGEs) are a family of molecules formed in the body through glycation reactions, and are known to be involved in inflammatory responses and oxidative stress. AGEs have been implicated not only in various chronic diseases but also in schizophrenia [3,4].
Against this background, the present study investigated the possibility that AGEs may partially mediate the relationship between bullying victimization and psychiatric symptoms during adolescence.
We first examined the association between bullying victimization at age 12 and pentosidine levels at age 14. Participants who had experienced bullying showed significantly higher pentosidine levels (adjusted β = 0.27, 95% CI 0.14–0.41, P < 0.001). This result suggests that bullying victimization, a form of social stress, may be associated with elevated pentosidine levels in the body.
We then examined the association between pentosidine levels at age 14 and psychiatric symptoms at age 16. Pentosidine levels were significantly associated with both psychosis-like experiences (adjusted β = 0.02, 95% CI 0.001–0.03, P < 0.01) and depressive symptoms (adjusted β = 0.21, 95% CI 0.09–0.32, P < 0.001).
Furthermore, causal mediation analysis was used to assess the mediating role of pentosidine in the relationship between bullying victimization and psychiatric symptoms. The results indicated that pentosidine mediated 28.0% of the association between bullying victimization and psychosis-like experiences, and 19.2% of the association between bullying victimization and depressive symptoms (Table).
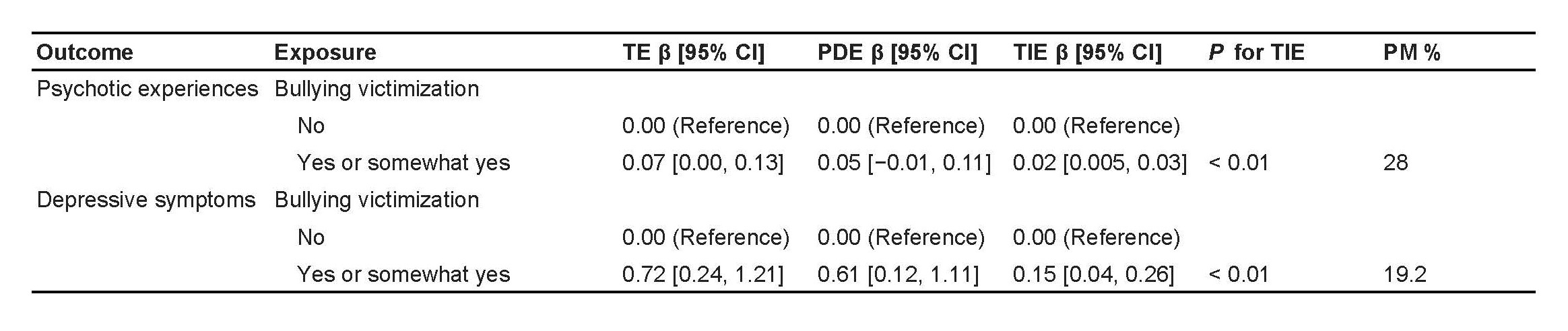
Missing data were handled using random forest imputation. PM was calculated by TIE/TE.
The model adjusted for age, sex, BMI, IQ, household income, loneliness, physical punishment, relationships with mother, father, and friends, neighborhood cohesion, gender nonconforming behavior, problematic internet use, pentosidine, and each mental health issue at age 12.
CIs were computed using the delta method.
TE: total effect, PDE: pure direct effect, TIE: total indirect effect, PM: proportion mediated, CI: confidence interval, BMI: body mass index, IQ: intelligence quotient.
Taken together, these findings suggest that bullying victimization during adolescence, as a social stressor, may influence psychiatric symptoms through glycation as a biological mechanism. This study is considered to contribute to our understanding of the biological processes linking social stress to subsequent psychiatric symptoms.
